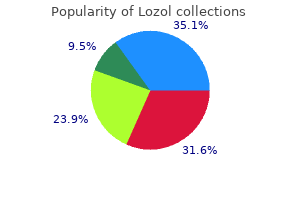
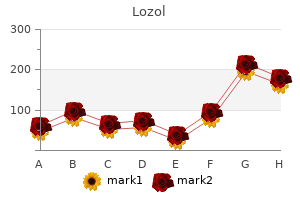
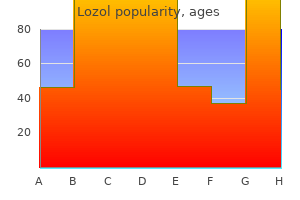
Lozol
"Generic lozol 2.5 mg without prescription, hypertension 14080".
By: X. Mamuk, M.A., Ph.D.
Vice Chair, Alabama College of Osteopathic Medicine
His mother and the two daughters carry the same mutation and were asymptomatic at the time of screening blood pressure keeps dropping proven 1.5mg lozol. Acroparesthesia or neuropathic pain in hands or feet beginning in later childhood blood pressure 40 year old woman discount lozol 2.5mg otc, precipitated by illness blood pressure ranges healthy purchase genuine lozol online, fever 5 fu arrhythmia buy generic lozol pills, exercise, emotional stress, or exposure to heat 2. This may be the only clinical manifestation of Fabry disease in patients of either gender with variants of classical Fabry disease. The 5-year survival after kidney transplantation is also lower than that of controls. However, Fabry nephropathy does not recur in the allograft, and transplanted Fabry patients appear to have better overall outcomes than those maintained on dialysis. Therefore, kidney transplantation should be recommended as a first choice therapy for patients with Fabry disease. It can be considered for every adult male patient, for symptomatic boys, and for symptomatic women. Two preparations are currently available, with other products in clinical development. In Elstein D, Altarescu G, Beck M, editors: Fabry disease, Dordrecht, Heidelberg, London, New York, 2010, Springer, pp. Fabrazyme is the only currently available enzyme replacement in the United States. Side effects of enzyme replacement therapy include fever, rigors, and chills, typically mild to moderate in nature. These occur in more than half of the patients during the first months of treatment. Infusion related reactions may be due to IgG or IgE antibodies that can be detected in several patients. In case of reactions, the infusion rate should be be decreased or stopped, and the administration of antihistamines and/or corticosteroids should be considered. Some patients need premedication with antihistamines, paracetamol/acetaminophen, or corticosteroids. In patients receiving maintenance dialysis therapy, the infusion can be administered during dialysis treatment. The clinical effect of both products was examined in two small pivotal trials, a few controlled studies, and numerous uncontrolled studies and registry reports. The primary endpoint was neuropathic pain that improved during therapy with Replagal as assessed by a pain questionnaire. After 20 weeks of treatment, 20 of the 29 patients (69%) in the Agalsidase B group had no microvascular endothelial Gb3 deposits, as compared to no clearance in the placebo group. Among secondary endpoints, there was no difference on pain between active treatment and placebo. A per-protocol analysis, adjusted for baseline proteinuria, however, suggested an effect of Agalsidase B as compared to placebo. Uncontrolled studies suggested stabilization or even improvement of renal and cardiac disease manifestations during enzyme replacement therapy in many patients. Quality of life, gastrointestinal symptoms, hypohydrosis, pulmonary obstruction, and other clinical symptoms also showed improvement. Kidney function, proteinuria, and blood pressure are important predictors of the renal response to enzyme replacement therapy. In a recent analysis of 213 treated patients (Agalsidase B for at least 2 years) enrolled in the Fabry Registry, a higher urinary protein level, poorer initial kidney function, and delayed initiation of enzyme replacement therapy after the onset of symptoms were strong predictors of kidney disease progression in men. Patients with 24-hour protein excretion greater than 1 g/24 h had poorer kidney function at baseline and follow-up compared with patients with protein excretion of 500 to 1000 mg/24 h or less than 500 mg/24 h. Kidney function was worse in patients with baseline hypertension, and there was a more rapid annual decline compared with normotensive patients. Taken together, these data clearly show that Agalsidase A or Agalsidase B cannot halt kidney disease progression in many patients. Thus, novel therapeutic strategies are needed to improve outcomes in patients with Fabry disease.
Pancreas formation the formation of the pancreas may be the flip side of liver formation hypertension 37 weeks pregnant order 2.5mg lozol free shipping. While the heart cells promote and the notochord prevents liver formation blood pressure kiosk for sale generic lozol 2.5 mg otc, the notochord may actively promote pancreas formation heart attack vs cardiac arrest purchase lozol 1.5 mg on-line, and the heart may block the pancreas from forming prehypertension numbers purchase cheap lozol online. It has been hypothesized (Gannon and Wright 1999) that the region of pdx1 expression in the endoderm endows a particular region of the digestive tube (including future portions of the stomach, duodenum, liver, and pancreas rudiments) with the ability to become either pancreas or liver. One set of conditions (presence of heart, absence of notochord) induces the liver, while another set of conditions (presence of notochord, absence of heart) causes the pancreas to form. The notochord activates pancreas development by repressing Sonic hedgehog expression in the endoderm (Apelqvist et al. Once the endodermal expression pattern of shh is established, the Pdx1 transcription factor becomes expressed in the pancreatic epithelium. If shh is experimentally expressed in this region, the tissue reverts to being intestinal. The pdx1 gene appears to give the pancreatic epithelium the ability to respond to its mesenchyme. Mice without this gene lack a pancreas, although their epithelium does differentiate into pre-islet cells that synthesize small amounts of glucagon and insulin (Jonnson et al. Once the pancreatic rudiments are initiated, they begin to form both exocrine and endocrine tissue. The exocrine tissue produces amylase and -fetoprotein, while the endocrine tissue makes insulin, glucagon, and somatostatin. The ratio of exocrine and endocrine cells is regulated by follistatin, a protein secreted by the pancreatic mesenchyme. The initial endocrine cells are thought to express the Pax6 and Pax4 transcription factors. The Pax6 transcription factor (in conjunction with Pdx1) may regulate both the expression of the pancreatic hormone genes (see Chapter 5) and the expression of adhesion proteins that link the endocrine cells together into the islets of Langerhans. Pax6-deficent mice have deficient pancreatic hormone production and malformed islets. Those cells that retain both Pax6 and Pax4 become the -cells of the islets of Langerhans, and they produce insulin. Those islet cells that down-regulate Pax4 and synthesize only Pax6 become the -cells that secrete glucagon (Sosa-Pineda et al. These transcription factors are important both for the morphogenesis of particular pancreatic cell types and for the expression of the hormone genes characteristic of the mature cell. Development of the tetrapod limb Pattern formation is the process by which embryonic cells form ordered spatial arrangements of differentiated tissues. The ability to carry out this process is one of the most dramatic properties of developing organisms, and one that has provoked a sense of awe in scientists and laypeople alike. How is it that the embryo is able not only to generate all the different cell types of the body, but also to produce them in a way that forms functional tissues and organs? It is one thing to differentiate the chondrocytes and osteocytes that synthesize the cartilage and bone matrices, respectively; it is another thing to produce those cells in a temporalspatial orientation that generates a functional bone. It is still another thing to make that bone a humerus and not a pelvis or a femur. The ability of limb cells to sense their relative positions and to differentiate with regard to those positions has been the subject of intense debate and experimentation. How are the cells that differentiate into the embryonic bone specified so as to form an appendage with digits at one end and a shoulder at the other? The vertebrate limb is an extremely complex organ with an asymmetrical arrangement of parts. There are three major axes to consider, one of which is the proximal (close) to distal (far) axis. The bones of the limb, be it wing, foot, hand, or flipper, consist of a proximal stylopod (humerus/femur) adjacent to the body wall, a zeugopod (radius-ulna/tibia-fibula) in the middle region, and a distal autopod (carpals-fingers/tarsals-toes) (Figure 16.
The direction of flow of cerebrospinal fluid is from the third to the Lateral Boundaries the caudal part of each lateral boundary is formed by the inferior cerebellar peduncle blood pressure 200 120 purchase lozol with mastercard. The cranial part of each lateral boundary is formed by the superior cerebellar peduncle arteria occipitalis order lozol cheap. Ventricular System 451 Longitudinal fissure Corpus callosum Genu of corpus callosum Frontal lobe Anterior horn of lateral ventricle Head of caudate nucleus Lentiform nucleus Olfactory tract Optic nerve Claustrum Lateral sulcus Insula Temporal lobe A Body of caudate nucleus Choroid plexus of lateral ventricle Thalamus (medial part) Thalamus (lateral part) Claustrum Putamen of lentiform nucleus Globus pallidus of lentiform nucleus Red nucleus Substantia nigra Longitudinal fissure Body of corpus callosum Septum pellucidum Body of lateral ventricle Body of fornix Third ventricle Insula Internal capsule Internal horn of lateral ventricle Cerebral aqueduct Superior colliculus Longitudinal fissure Splenium of corpus callosum Tapetum of corpus callosum Optic radiation Posterior horn of lateral ventricle Region of collateral eminence Calcarine sulcus Collateral sulcus Calcar avis Inferior longitudinal bundle B Choroid plexus C Figure 16-5 Coronal sections of the brain passing through the anterior horn of the lateral ventricle (A) pulse pressure sensor order genuine lozol online, the body of the lateral ventricle (B) hypertension uncontrolled cheap 2.5mg lozol mastercard, and the posterior horn of the lateral ventricle (C). Midbrain Ependyma Arachnoid mater Pia mater Subarachnoid space filled with cerebrospinal fluid Pons Pontine cistern Cavity of fourth ventricle filled with cerebrospinal fluid Choroid plexus of fourth ventricle Cerebellum Cerebellomedullary cistern Median opening in roof of fourth ventricle (foramen of Magendie) Central canal Medulla oblongata Figure 16-7 Sagittal section of the fourth ventricle showing the origin and circulation of the cerebrospinal fluid. Ventricular System 453 Corpus callosum Body of fornix Pia mater Corpus callosum Ependyma Cavity of lateral ventricle Choroid plexus of lateral ventricle Caudate nucleus Thalamus Pia mater of tela choroidea in roof of third ventricle Choroid plexus of third ventricle Cavity of third ventricle Ependyma A Choroid fissure Fimbria Dentate gyrus Pia mater Choroid plexus of lateral ventricle Cavity of inferior horn of lateral ventricle Ependyma Pia mater Medial Lateral Parahippocampal Parahippocampal gyrus gyrus Hippocampus Lateral occipitotemporal Lateral occipitotempora gyrus gyrus Collateral sulcus B Figure 16-8 Coronal section of the cavities of the third and lateral ventricles (A) and the cavity of the inferior horn of the lateral ventricle (B). The superior part is formed by the medial borders of the two superior cerebellar peduncles and a connecting sheet of white matter called the superior medullary velum. The inferior part of the roof is formed by the inferior medullary velum, which consists of a thin sheet devoid of nervous tissue and formed by the ventricular ependyma and its posterior covering of pia mater. This part of the roof is pierced in the midline by a large aperture, the median aperture or foramen of Magendie. Lateral recesses extend laterally around the sides of the medulla and open anteriorly as the lateral openings of the fourth ventricle, or the foramina of Luschka. Thus, the cavity of the fourth ventricle communicates with the subarachnoid space through a single median opening and two lateral apertures. These important openings permit the cerebrospinal fluid to flow from the ventricular system into the subarachnoid space. Floor or Rhomboid Fossa the diamond-shaped floor is formed by the posterior surface of the pons and the cranial half of the medulla oblongata. On each side of this sulcus, there is an elevation, the medial eminence, which is Cerebral aqueduct Midbrain Superior colliculus Inferior colliculus Superior medullary velum Lingula Cerebral peduncle Central lobule Culmen Primary fissure Oculomotor nerve Declive Folium Pons Cavity of fourth ventricle Roof of fourth ventricle and choroid plexus Medulla oblongata Horizontal fissure Tuber Cerebellar hemisphere Nodule Pyramid Median aperture in roof of fourth ventricle (inferior medullary velum) Central canal Uvula Tonsil Cortex of cerebellum Figure 16-9 Sagittal section through the brainstem and the cerebellum showing the fourth ventricle. Substantia ferruginea Trochlear nerve Midbrain Median sulcus Superior cerebellar peduncle Medial eminence Sulcus limitans Vestibular area Facial colliculus Middle cerebellar peduncle Pons Striae medullares Inferior cerebellar peduncle Medulla oblongata Figure 16-10 Posterior surface of the brainstem showing the floor of the fourth ventricle. A: the vermis of the cerebellum has been divided in the midline, and the cerebellar hemispheres have been displaced laterally. B: the greater part of the cerebellum has been removed, leaving the superior and inferior medullary vela. Note that the right half of the inferior medullary velum has been reflected inferiorly to reveal the choroid plexus. Lateral to the sulcus limitans, there is an area known as the vestibular area. The facial colliculus is a slight swelling at the inferior end of the medial eminence that is produced by the fibers from the motor nucleus of the facial nerve looping over the abducens nucleus. At the superior end of the sulcus limitans, there is a bluish-gray area, produced by a cluster of nerve cells containing melanin pigment; the cluster of cells is called the substantia ferruginea. Strands of nerve fibers,the stria medullaris, derived from the arcuate nuclei, emerge from the median sulcus and pass laterally over the medial eminence and the vestibular area and enter the inferior cerebellar peduncle to reach the cerebellum. The cerebellum has been displaced superiorly to show the large median aperture (foramen of Magendie). Inferior to the stria medullaris, the following features should be recognized in the floor of the ventricle. The most medial is the hypoglossal triangle, which indicates the position of the underlying hypoglossal nucleus. Lateral to this is the vagal triangle, beneath which lies the dorsal motor nucleus of the vagus. The area postrema is a narrow area between the vagal triangle and the lateral margin of the ventricle, just rostral to the opening into the cen- tral canal. Choroid Plexus of the Fourth Ventricle the choroid plexus has a T shape; the vertical part of the this double. It is suspended from the inferior half of the roof of the ventricle and is formed from the highly Inferior colliculus Trochlear nerve Superior medullary velum Roof of fourth ventricle Nodule of cerebellum Part of cerebellar hemisphere (cut) Superior cerebellar peduncle Dentate nucleus of cerebellum Lateral recess of fourth ventricle (showing lateral aperture) Inferior cerebellar peduncle Cuneate tubercle Median aperture (opening into fourth ventricle) Central canal Gracile tubercle Figure 16-13 Posterior view of the roof of the fourth ventricle after removal of the greater part of the cerebellum. Subarachnoid Space 457 Fourth ventricle Motor nucleus of abducent nerve Nucleus solitarius of facial nerve Superior salivatory nucleus of facial nerve (parasympathetic) Motor nucleus of facial nerve Transverse pontine fibers Corticospinal and corticonuclear fibers Figure 16-14 Transverse section through the fourth ventricle and the pons showing the nuclei of the facial nerve and their relationship to the nucleus of the abducent nerve. The tela choroidea is a two-layered fold of pia mater that projects through the roof of the ventricle and is covered by ependyma. The blood supply to the plexus is from the posterior inferior cerebellar arteries.
Syndromes
- Increased sweating
- Treatments to water down (dilute) the acid
- Electromyography to see which nerves or muscles do not work properly
- 99 °F (37.2 °C) measured under the arm (axillary)
- Pulmonary edema
- Include a maintenance program and other support and referral resources to reinforce the new behaviors and to deal with underlying issues that contributed to overweight.
- Corticosteroids
- Antibiotics given to food producing animals
- Enlarged heart
In young women arrhythmia lidocaine cheap lozol 1.5 mg visa, conservative surgery hypertension fact sheet discount lozol on line, either ovarian cystectomy or ovariotomy (oophorectomy) is to be done arrhythmia genetic trusted 1.5 mg lozol. In patient around 40 years and above blood pressure ranges pediatrics lozol 2.5 mg visa, total hysterectomy with bilateral salpingo-oophorectomy is justified. In elderly women total hysterectomy, bilateral salpingo-oophorectomy and omentectomy are done. In all cases, the tumor is subjected to histopathological study to note the nature of the tumor and to exclude malignancy. These ectopic endometrial tissues may be found in the myometrium when it is called endometriosis interna or adenomyosis. More commonly, however, these tissues are found at sites other than uterus and are called endometriosis externa or generally referred to as endometriosis. PrEvalEncE During the last couple of decades, the prevalence of endometriosis has been increasing both in terms of real and apparent. The real one is due to delayed marriage, postponement of first conception and adoption of small family norm. The apparent one is due to increased use of diagnostic laparoscopy as well as hightened awareness of this disease complex amongst the gynecologists. However, prevalence is high amongst the infertile women (3040%) as based on diagnostic laparoscopy and laparotomy. Extra-abdominal: the common sites are abdominal scar of hysterotomy, cesarean section, tubectomy and myomectomy, umbilicus, episiotomy scar, vagina and cervix. The endometrial fragments get implanted in the peritoneal surface of the pelvic organs (dependent sites. Subsequently, cyclic growth and shedding of the endometrium at the ectopic sites occur under the influence of the endogenous ovarian hormones. Probably, a genetic factor or favorable hormonal milieu is necessary for successful implantation and growth of the fragments of endometrium. While this theory can explain pelvic endometriosis, it fails to explain the endometriosis at distant sites. Coelomic metaplasia (Meyer and ivanoff) Chronic irritation of the pelvic peritoneum by the menstrual blood may cause coelomic metaplasia which results in endometriosis. Alternatively, the mьllerian tissue remnants may be trapped within the peritoneum. Direct implantation According to the theory, the endometrial or decidual tissues start to grow in susceptible individual when implanted in the new sites. Such sites are abdominal scar following hysterotomy, caesarean section, tubectomy and myomectomy. Endometriosis at the episiotomy scar, vaginal or cervical site can also be explained with this theory. This theory however, fails to clarify endometriosis at sites other than mentioned. Lymphatic theory (halban): It may be possible for the normal endometrium to metastasize the pelvic lymph nodes through the draining lymphatic channels of the uterus. Vascular theory: this is sound at least to explain endometriosis at distant sites such as lungs, arms or thighs. However, a defect of local cellular immunity may be responsible for the ectopic tissue to grow in abnormal sites only in susceptible women. Furthermore activated macrophages reduce sperm motility, increase sperm phagocytosis and interfere with fertilization. Environment theory suggests somatic mutations of cells due to environmental factors (pollutants, dioxins). Ovarian and deep infiltrating endometriotic lesions are explained with this theory. Thus, it is certain that, not all cases of endometriosis at different sites can be explained by a single theory.
Buy generic lozol from india. Does a High Fiber Diet Lower Your Blood Pressure? (Yes or No?).