Capoten
"Capoten 25 mg line, medications you can crush".
By: S. Roy, M.A., M.D., Ph.D.
Assistant Professor, Charles R. Drew University of Medicine and Science
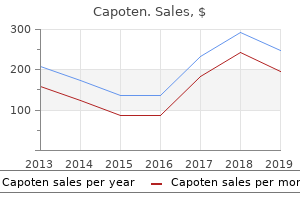
Oral aspirin (75 to 325 mg/day) produces its antithrombotic effects by irreversibly blocking platelet cyclooxygenase and treatment kidney failure capoten 25 mg on-line, consequently medicine symbol order capoten online from canada, thromboxane A2 -dependent platelet recruitment (see Chapter 29) treatment pancreatitis order capoten 25 mg line. Clopidogrel has none of the troublesome adverse effects plaguing ticlopidine and is at least as safe as moderate-dose aspirin (325 mg/day) symptoms liver disease buy capoten master card. Because aspirin and clopidogrel inactivate separate pathways of platelet recruitment, combined aspirin and clopidogrel are predicted to produce additive antithrombotic effects. This postulate is strongly supported by pre-clinical findings, as well as by the enhanced antithrombotic effects produced by aspirin and ticlopidine in patients undergoing endovascular stenting. Clinical trials are presently evaluating the potential usefulness of combined aspirin and clopidogrel. Because these agents also impair platelet hemostatic function, their use is generally reserved for transient interruption of high-risk thrombosis. Three fibrinogen receptor antagonists are presently available for parenteral use: abciximab (humanized monoclonal antibody), eptifibatide (synthetic cyclic peptide), and tirofiban (synthetic antagonist). Aspirin, clopidogrel, or ticlopidine decrease the risk of thrombo-occlusion and thromboembolism for all major vascular distributions, irrespective of the anatomic site producing symptoms (Table 188-2). Although aspirin therapy is associated with a small increase in hemorrhagic stroke, the overall reduction in all strokes far outweighs that complication. Although dipyridamole has recently been reported to enhance the effects of aspirin, this outcome is inconsistent with previous controlled trials reporting that aspirin alone produces equivalent outcomes to the combination of aspirin and dipyridamole and that dipyridamole alone fails to prevent subsequent stroke when compared with placebo. Although there is much less experience in acute ischemic coronary syndromes, the available evidence suggests that clopidogrel or ticlopidine may exhibit similar effects. Free and fibrin-bound thrombin is inactivated by direct thrombin inhibitors such as hirudin, bivalirudin, or argatroban. These agents effectively block platelet recruitment into the thrombus, regardless of the inducing mechanism (see Fig. Because effective antithrombotic doses of these agents concurrently inhibit platelet hemostasis, abnormal bleeding may complicate their use, particularly in association with invasive procedures. To maintain graft patency without increasing surgical bleeding, patients undergoing saphenous vein or internal mammary artery aortocoronary grafting should receive aspirin (325 mg/day) within hours after completing the procedure and continue aspirin therapy for 1 year. Nevertheless, aspirin is often recommended in individuals whose principal risk is coronary artery disease (see Chapters 59 and 60). Low-dose aspirin (100 mg daily) and oral anticoagulation are more effective than coumarin anticoagulants alone in reducing the thromboembolic complications of mechanical heart valves (see Chapter 63). However, adding aspirin to anticoagulant therapy increases the incidence of serious gastrointestinal bleeding when the dose of aspirin exceeeds 100 mg/day. When aspirin fails or is contraindicated, dipyridamole (100 mg four times daily) in combination with oral anticoagulant therapy is currently recommended in patients with mechanical heart valves in the aortic and mitral positions. Alternatively, ticlopidine (or clopidogrel) may also be used in addition to oral anticoagulation to reduce thromboembolic occlusive events complicating the placement of mechanical heart valves. The combination of aspirin and ticlopidine (or clopidogrel) reduces vascular occlusive events in patients with peripheral vascular disease who are undergoing grafting procedures and in hemodialysis patients receiving arteriovenous access grafts. However, these therapies fail to decrease the formation of stenotic anastomotic vascular lesion formation, which is the principal underlying cause of graft failure. Combining aspirin and ticlopidine (or presumably aspirin and clopidogrel) therapy for several weeks following the deployment of coronary artery endovascular stents substantially decreases stent thrombotic vascular occlusion when compared with aspirin alone (see Chapter 61). Thrombo-occlusive events complicate coronary angioplasty in high-risk patients despite treatment with aspirin and heparin (See Chapters 61). Resistance to aspirin is explained by the dominance of thrombin, as opposed to thromboxane A2 in mediating the thrombogenic process initiated by mechanical vascular injury. Resistance to heparin is attributable to the inaccessibility of bound thrombin to inhibition by the heparin-antithrombin complex, together with the local heparin-inhibiting effects of proteins secreted by activated platelets (platelet factor 4). By blocking this final common pathway regulating platelet recruitment, the participation of platelets in thrombus formation is abolished. Aspirin at 1 mg/kg is as effective as higher doses in the majority of patients at risk. Because just 10% non-aspirin-treated platelets in the circulation are sufficient to generate full thromboxane A2 -dependent platelet aggregation in the blood of aspirin-treated patients, aspirin should be given every day to inhibit newly formed platelets. Larger doses of aspirin (1 g/day) have been recommended for stroke-prone patients by some neurologists, who reason that dose-response data are inadequate in stroke trials and platelet aggregation results suggest the possibility of resistance to aspirin inhibition. However, because the gastrointestinal complications of aspirin are dose dependent, most practitioners prescribe daily aspirin at a dose of 75 to 325 mg. Ticlopidine in combination with aspirin is currently used in patients undergoing coronary artery stenting.
Monosodium urate crystals are rods or needles up to 15 to 20 mum in length and are brightly birefringent with negative elongation when viewed with compensated polarized light medicine klonopin purchase capoten without prescription. Those from visible tophi or synovial microtophi tend to be more often needle-like medicine 48 12 cheap capoten 25mg visa, whereas some in acute arthritis can be very short symptoms xanax cheap capoten online. Leukocyte counts during attacks usually range from 10 symptoms 8dp5dt buy capoten uk,000 to 50,000 per cubic millimeter, with 80 to 90% neutrophils. Gout is most common in middle-aged men but is increasingly seen in women after menopause. A variety of lower extremity joints are commonly involved, in addition to the classic first metatarsophalangeal joint, but any joint or bursa, including those in the upper extremities, can be affected by either acute or chronic arthritis. Chronic or recurrent acute gout can be polyarticular, can mimic rheumatoid arthritis, and may be misdiagnosed, especially if the typical dramatic early short-lived attacks are not appreciated and synovial fluid is not examined. Crystals are often present in joint fluid even between attacks and may contribute to low-grade inflammation and joint damage. Radiographs show only soft tissue swelling early in gout but can later reveal cystic erosions with thin, overhanging edges of bone suggestive of gout. Soft tissue tophi are common around joints, in bursae, in Achilles tendons, and at the extensor surface of the forearm. Gout should be recognized as a syndrome resulting from the many possible causes noted in Chapter 299. Cyclosporine causes an especially rapidly progressive form of gout in transplant patients. The latter two agents may be needed in complicated patients with renal failure, liver disease, or gastrointestinal disease. Joint aspiration with instillation of depot corticosteroids may also be used if a single joint is involved and infection is excluded. Thus with more frequent attacks or visible tophi, patients should be considered for long-term lowering of urate levels with a uricosuric agent such as probenecid (if renal function is good and the patient is not overexcreting uric acid) or, in other cases, allopurinol, a xanthine oxidase inhibitor. Either urate-lowering agent must be given in sufficient dosage to lower serum uric acid levels below 6. Some of the complex situations involved in colchicine use for acute and chronic gout are reviewed. The uncommon disease relapsing polychondritis is characterized by recurrent inflammation and destruction of cartilaginous and other connective tissue structures. Frequently involved cartilagenous structures are the pinnae of the ears, nasal cartilage, and tracheal rings. Polychondritis occurs nearly equally in both genders and at any age, but with a peak in onset between the ages of 40 and 60. The pathologic lesion seen by light microscopy consists of loss of matrix staining, predominantly superficial infiltration with polymorphonuclear neutrophils or lymphocytes, and eventual destruction of normal structures followed by fibrosis. Electron microscopy in addition shows alterations of superficial chondrocytes, matrix, and elastic fibers. The cause of polychondritis is unknown, but the location of lesions and frequency of associated systemic diseases suggest the importance of systemic factors. Inflammation of the cartilaginous structures of the ears is the most common initial finding (see Color Plate 8 C). An acute onset of pain and tenderness may be seen along with erythema and swelling of one or both helices. Laryngeal and tracheal disease can cause hoarseness or life-threatening upper respiratory obstruction. Ocular manifestations are common and include conjunctivitis, episcleritis, iridocyclitis, proptosis, and, rarely, other problems such as optic neuritis. Cardiac involvement, especially involvement of the aortic root with aortic insufficiency, is seen in up to one fourth of cases. Arthritis is reported in about three fourths of cases but is generally non-destructive. No laboratory tests are diagnostic, although the erythrocyte sedimentation rate is often elevated.
Discount 25mg capoten with visa. Fetal Heart Rate Tone Monitoring Decelerations | Early Late Variable NCLEX OB Maternity Nursing.
Thus melatonin-which is produced only during the night-may be the chemical messenger of darkness symptoms 5 days after iui order cheapest capoten. Therefore symptoms hyperthyroidism purchase 25mg capoten visa, human melatonin production may normally have a role medications 2355 buy capoten mastercard, however small symptoms 5 months pregnant buy capoten toronto, in entrainment of the circadian rhythms of the suprachiasmatic nuclei. Not being seasonal breeders, perhaps humans have retained the suppressant effect of light in order to use endogenous melatonin to more effectively augment the entrainment and phase-shifting effects of the light/dark cycle. Symptomatic enlargement of the pineal gland by cysts has also been reported, but these conditions are almost always asymptomatic. Destruction of pineal tissue can reduce or even ablate melatonin production, but pineocytomas have rarely been associated with increased circulating levels of melatonin. Melatonin production decreases with age, but this decrease does not seem to be related to pineal calcification. By occluding the cerebral aqueduct, pineal tumors can produce symptoms associated with increased intracranial pressure, sometimes necessitating a shunt. Some germinomas and embryonal carcinomas secrete human chorionic gonadotropin, which has been implicated in cases of delayed onset of puberty. Treatment modalities include surgical extirpation, radiation, and chemotherapy, depending on tumor type and location and the absence or degree of metastases. The pituitary is divided into anterior and posterior lobes, with the anterior lobe comprising about 80% of the gland. The posterior pituitary or neurohypophysis consists of the pituitary stalk as well as the posterior lobe (see Chapter 238). Superiorly, the pituitary is covered by the diaphragma sella, a reflection of the dura mater that forms the roof of the sella and is attached to the clinoid processes. The diaphragma sella has a central opening that is penetrated by the pituitary stalk and its blood vessels. Importantly, the optic chiasm, formed by the decussation of the optic nerves, is positioned directly above the pituitary gland and below the third ventricle. The exact position of the chiasm is variable, affecting the pattern of visual field changes experienced by patients with pituitary tumors that expand into the suprasellar region. The blood supply to the pituitary gland is derived from the superior and inferior hypophyseal arteries, branches of the internal carotid arteries. Specialized vascular structures, referred to as gomitoli, are located in the median eminence of the hypothalamus and consist of short terminal arterioles that drain into portal veins that course down the pituitary stalk to join the sinusoidal capillaries of the anterior lobe. Hypothalamic hormones enter fenestrations in the perigomitolar capillaries to flow from the hypothalamus to the anterior pituitary. Venous drainage from the anterior lobe enters the posterior pituitary capillary bed before draining into the cavernous sinuses. The cavernous sinuses are interconnected by means of channels that encircle the pituitary, and they drain into the petrosal sinuses. The biochemical characteristics of the major anterior pituitary hormones are summarized in Table 237-1. However, there is some evidence that the anterior pituitary may develop from a more rostral neuroectoderm fold rather than this ectodermal tissue. The ontogeny of hormone production during anterior pituitary development has been characterized in detail. The transcription factor Pit-1, a member of the Pou-Homeodomain family, is produced in somatotrophs, lactotrophs, and thyrotrophs. Anterior pituitary hormone production is largely established by the ninth week of gestation, and the anatomic and biosynthetic mechanisms that comprise an active hypothalamic-pituitary system appear to be functional by 12 to 17 weeks of gestation. In anencephaly, all anterior pituitary cell types, with the exception of corticotrophs, are capable of hormone synthesis and secretion, indicating that the embryonic pituitary develops relatively normally in the absence of hypothalamic stimulation. Somatotrophs, which constitute 40 to 50%, and lactotrophs, which make up 15 to 25%, of anterior pituitary cells, are located predominantly in the lateral aspects of the anterior pituitary. Corticotrophs constitute 10 to 20% of anterior pituitary cells and are located mainly in the central region of the anterior pituitary. The folliculostellate cells have long irregular processes that extend between the hormone-producing cells. They do not contain secretory granules but have been shown to produce growth factors such as basic fibroblast growth factor, vascular endothelial growth factor, and follistatin, among others. The normal anterior pituitary appears isointense with brain white matter, whereas the posterior pituitary exhibits high signal intensity.
Whereas the elevated calcitriol level underlies increased gastrointestinal absorption of calcium and hypercalciuria in these diseases treatment ringworm purchase genuine capoten line, the impact of abnormal vitamin D metabolism on the phenotypic expression of the phosphopenic disorders is less certain red carpet treatment order capoten now. In those diseases with normal serum calcium and phosphorus concentrations medications like prozac discount capoten 25 mg mastercard, laboratory abnormalities are unique to each form of the disease symptoms zoloft withdrawal generic 25 mg capoten with amex. Nevertheless, alkaline phosphatase activity in plasma is generally elevated in all forms of rickets and osteomalacia. Even severe forms of disease, however, particularly those due to renal tubular disorders, may be associated with normal or only marginally elevated enzyme activity. The variable biochemical abnormalities associated with these disparate disorders are summarized in Table 263-2. Although many of these diseases are no longer common causes of rickets and osteomalacia, others are often hidden causes of bone disease in a varying population of patients. Adequate exposure to sunlight and fortification of dairy products with vitamin D have eliminated vitamin D deficiency secondary to inadequate endogenous production or nutrition in the majority of countries. However, in several populations, such as Asian immigrants in Britain, rickets and osteomalacia secondary to vitamin D deficiency occurs in neonates and infants, adolescents during pubertal growth, and less frequently among adults. Insufficient vitamin D intake secondary to using unfortified foods, racial pigmentation (which interferes with ultraviolet transmission through the skin), genetic factors, and social customs (such as avoiding sun exposure) contribute to the development of disease in these subjects. Moreover, in the United States and other developed countries, a surprisingly frequent occurrence of vitamin D deficiency osteomalacia has been recognized recently in alcoholics, institutionalized patients, and the elderly. Poor diet, in some cases including avoiding milk and milk products due to lactose intolerance, lack of sunlight exposure, and an age-related decline in the dermal synthesis of 7-dehydrocholesterol are among the factors predisposing to the vitamin D deficiency and consequent bone disease. Measurement of this metabolite therefore serves to identify populations at risk for and facilitates early detection of vitamin D deficiency rickets and osteomalacia. Introducing vitamin D supplements (400 U/day) may, under these circumstances, prevent development of clinically significant disease. Regardless, treating clinically evident vitamin D-deficient rickets and osteomalacia invariably results in healing of the bone disease. The disorder is best treated with vitamin D and restoration of normal dietary calcium and phosphorus intake. Ergocalciferol (vitamin D2) is preferred because it provides the missing substrate that submits to physiologic regulation of vitamin D metabolite production. In general, malabsorption of vitamin D occurs as a consequence of steatorrhea, which disturbs fat emulsification and chylomicron-facilitated absorption (see Chapter 134). However, most affected patients are asymptomatic, and many exhibit only reduced bone volume rather than evidence of defective bone mineralization. Intestinal bypass surgery and adult celiac disease are common examples of disorders in which vitamin D malabsorption occurs and in which the suspicion for osteomalacia should remain high. In contrast, patients with cholestatic liver disease, extrahepatic biliary obstruction, and diseases of the distal portions of the small intestine, such as regional enteritis, may develop bone disease secondary not only to poor vitamin D absorption but to disruption of enterohepatic circulation as well. Osteomalacia may also develop in patients who have had partial or total gastrectomy for peptic ulcer disease or other indications. Loss of gastrointestinal acidity or malfunction of the proximal small bowel underlies the vitamin D malabsorption in such circumstances. Absence of sufficient absorbing surface or failure of intestinal mucosal cells to respond to vitamin D or its metabolites may also cause vitamin D malabsorption and consequent bone disease. The prevalence of osteomalacia in patients with gastrointestinal malabsorption varies widely from country to country. However, as many as 25 to 50% of British and European patients with partial gastrectomy, inflammatory bowel disease, and cholestatic liver disease have bone biopsy-proven osteomalacia. Treatment of established disease generally requires pharmacologic amounts of vitamin D or its metabolites to overcome the defective absorption and the aberrant enterohepatic circulation or to offset end-organ resistance at the intestinal mucosa. If the severity of malabsorption makes oral vitamin D ineffective, parenteral ergocalciferol, 12,500 to 25,000 mug, given intramuscularly once a month, is a practical alternative. Because magnesium deficiency often co-exists in malabsorptive diseases and may slow healing of the osteomalacia, adjunctive therapy with magnesium oxide may facilitate bone mineralization. These patients, however, rarely manifest biochemical or histologic evidence of osteomalacia.