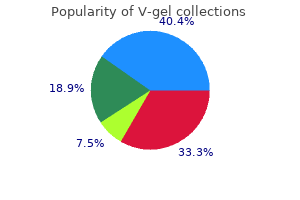
V-gel
"Order 30gm v-gel with amex, earthworm herbals".
By: O. Dennis, M.A.S., M.D.
Clinical Director, Northwestern University Feinberg School of Medicine
Posttraumatic Hydrocephalus this is an uncommon complication of severe head injury earthsong herbals buy generic v-gel from india. Intermittent headaches herbals and surgery cheap v-gel 30gm line, vomiting herbs not to mix trusted 30 gm v-gel, confusion herbs lower blood pressure buy v-gel 30 gm on line, and drowsiness are the initial manifestations. Since a similar syndrome is observed occasionally after the rupture of a saccular aneurysm with subarachnoid hemorrhage, the same mechanisms, i. Zander and Foroglou have had extensive experience with this condition and have written informatively about it. Posttraumatic Nervous Instability (Postconcussion Syndrome) this troublesome and frequent sequela of head injury has been mentioned above as well as in the chapter on headache (page 158). When the syndrome is protracted, neurologists are vexed by the condition- a problem intensified by worried patients and family. It has also been called the posttraumatic or postconcussion syndrome, posttraumatic headache, traumatic neurasthenia (Symonds), and traumatic psychasthenia, among many other names. Headache is the central symptom, either generalized or localized to the part that had been struck. The headache is variously described as aching, throbbing, pounding, stabbing, pressing, or band-like and is remarkable for its variability. The intensification of the headache and other symptoms by mental and physical effort, straining, stooping, and emotional excitement has been mentioned earlier; rest and quiet tend to relieve it. Dizziness, another prominent symptom, is usually not a true vertigo but a giddiness or lightheadedness. However, a certain number of patients describe symptoms that are consonant with labyrinthine disorder. They report that objects in the environment move momentarily, and that looking upward or to the side may cause a sense of unbalance; labyrinthine tests may show hyporeactivity; far more often they disclose no abnormalities. McHugh found a high incidence of minor abnormalities by electronystagmography both in concussed patients and in those suffering from whiplash injuries of the neck; but we find some of the data difficult to interpret. Exceptionally, vertigo is accompanied by diminished excitability of both the labyrinth and the cochlea (deafness), and one may assume the existence of direct injury to the eighth nerve or end organ. When the symptoms persist, however, the patient is intolerant of noise, emotional excitement, and crowds. Tenseness, restlessness, fragmentation of sleep, inability to concentrate, feelings of nervousness, fatigue, worry, apprehension, and an inability to tolerate the usual amount of alcohol complete the clinical picture. The resemblance of these symptoms to those of anxiety and depression and to other forms of "posttraumatic stress disorder" is quite apparent. In contrast to this multiplicity of subjective symptoms, memory and other intellectual functions show little or no impairment, although this has been disputed. Leininger et al, for example, found that most of their 53 patients who suffered minor head injury in traffic accidents performed less well than controls on psychologic tests (category test, auditory verbal learning, copying of complex figures). The fact that those who were merely dazed did as poorly as those who were concussed and that litigation was involved in some cases would lead one to question these results. The syndrome of posttraumatic nervous instability complicates all types of head injury, mild and severe. Once established, it may persist for months or even years, and it tends to resist all varieties of treatment. Characteristic also is the augmentation of both the duration and intensity of this syndrome by problems with compensation and litigation, suggesting a psychologic factor. In countries where these matters are a less prominent part of the social fabric, the occurrence of posttraumatic syndrome is far less frequent. Stable, athletic, tough-fibered individuals take a concussive injury in stride, while the sensitive, nervous, complaining types may be so overwhelmed by such an accident that they are unable to expel it from their minds. Environmental stress assumes importance as well, for if too much is demanded of the patient soon after injury, irritability, insomnia, and anxiety are enhanced. In this connection, an interesting experiment was conducted by Mittenberg and colleagues.
In individuals so exposed there occurs a gradual weakening of the legs accompanied by spasticity and cramps wicked herbals cheap 30 gm v-gel with visa. These symptoms herbals shops cheap v-gel 30gm otc, once established herbals products order v-gel 30 gm with amex, are more or less permanent but not constantly progressive jeevan herbals hair oil order v-gel us, and most of the patients live out their natural life span. Only two reports on the neuropathology of lathyrism were known to Dastur, one by Buzzard and Greenfield in England, the other by Filiminoff in Russia. Greenfield noted a loss of ascending and descending tracts in the spinal cord, particularly the corticospinal and direct spinocerebellar tracts. Filiminoff observed a loss of myelinated fibers in the lateral and posterior columns. Unlike the cases of Spencer et al, there had been a loss of pain and thermal sensation in the upper extremities. The toxic nature of this disease, long suspected, was confirmed by Spencer and colleagues. Subsequently, Hugon and coworkers produced a primate model of lathyrism by feeding monkeys a diet of L. These findings tend to negate the importance of several other factors that until now had been thought to be causative- namely, malnutrition, ergot contamination, and toxins derived from Vicia sativa, the common vetch that grows alongside the lathyrus species. The African acute spastic paraplegia called "konzo" has a similar toxic pathogenesis; it is caused by cyanide-like compounds in flour made from cassava. Pathologically there is cavitation of the central parts of the spinal cord, usually in the cervical region, but extending upward in some cases into the medulla oblongata and pons (syringobulbia) or downward into the thoracic or even the lumbar segments. Frequently there are associated developmental abnormalities of the vertebral column (thoracic scoliosis, fusion of vertebrae, or Klippel-Feil anomaly), of the base of the skull (platybasia and basilar invagination), and particularly of the cerebellum and brainstem (type I Chiari malformation). Approximately 90 percent of cases of syringomyelia have type I Chiari malformation consisting of a descent of cerebellar tonsils (see page 861). Conversely, approximately 50 percent of type I Chiari malformations are associated with syringomyelia. There is also a group of less frequent but well-described syringomyelias that derives from the acquired processes mentioned earlier such as intramedullary tumor (astrocytoma, hemangioblastoma, ependymoma) and traumatic or hemorrhagic necrosis of the spinal cord. Wider experience with the pathology of the developmental type of syringomyelia and better understanding of the postulated mechanisms have led to the following classification, modified from Barnett and colleagues: Type I. Syringomyelia with obstruction of the foramen magnum and dilation of the central canal (developmental type) A. Later, following recognition of the central canal as a normal structure, it was assumed by Vir- Dysraphic Syndromes (Spina Bifida) and Tethered Cord these are described in Chap. The pattern of inheritance in almost all our adult cases has been autosomal dominant. A lack of sensory symptoms and signs and sparing of sphincteric function until late in the illness are important diagnostic features. A number of adult cases are "complicated" in the sense that the spastic paraplegia is associated with cerebellar ataxia or dementia. By contrast, primary lateral sclerosis, a sporadic form of degenerative disease of the motor system, is characterized by a pure spastic paraplegia and bulbar spastic palsy either initially or with progression, the result of changes that are confined to the corticospinal pathways. These disorders are discussed extensively with the heredodegenerative diseases in Chap. Cavities in the central portions of the spinal cord, unconnected with the central canal, were recognized by Hallopeau (1870); Simon suggested in 1875 that the term syringomyelia be reserved for such cavities and that the term hydromyelia be restricted to simple dilatation of the central canal. Thus, a century ago, the stage was set for an argument about pathogenesis that has not been settled to the present day. Clinical Features the clinical picture varies in the four pathologic types previously listed, the differences depending not only on the extent of the syrinx but also on the associated pathologic changes, particularly those related to the Chiari malformation. In the classic type 1 syrinx (idiopathic and Chiari developmental syringomyelia) symptoms usually begin in early adult life (20 to 40 years). Rarely, some abnormality is noted at birth, but usually the first symptom appears in late childhood or adolescence. In many instances the symptoms or signs are discovered accidentally, for example as a result of painless burn or atrophy of the hand, and the patient cannot say when the disease began. Rarely, there is an almost apoplectic onset or worsening; there are cases on record of an aggravation of old symptoms or the appearance of new symptoms after a violent strain or paroxysm of coughing.
Surgical removal is supplemented by radiation therapy herbals 30gm v-gel for sale, particularly to address the high rate of seeding of the ventricles and spinal axis wicked x herbal order generic v-gel line. In the treatment of cerebral ependymoblastomas zever herbals buy v-gel us, antitumor drugs are often used in combination with radiation therapy herbals dario bottineau purchase 30 gm v-gel. Meningioma (See also page 577) this is a benign tumor, first illustrated by Matthew Bailie in his Morbid Anatomy (1787) and first recognized by Bright, in 1831, as originating from the dura mater or arachnoid. It was analyzed from every point of view by Harvey Cushing and was the subject of one of his most important monographs. Meningiomas represent about 15 percent of all primary intracranial tumors; they are more common in women than in men (2:1) and have their highest incidence in the sixth and seventh decades. There is evidence that persons who have undergone radiation therapy to the scalp or cranium are vulnerable to the development of meningiomas and that the tumors appear at an earlier age in such individuals (Rubinstein et al). There are a number of reports of a meningioma developing at the site of previous trauma, such as a fracture line, but the association is uncertain. The most frequent genetic defects of meningiomas are truncating (inactivating) mutations in the neurofibromatosis 2 gene (merlin) on chromosome 22q. Merlin deletions probably also play a role in those instances in which there is a loss of the long arm of chromosome 22. Meningiomas also elaborate a variety of soluble proteins, some of which (vascular endothelial growth factor) are angiogenic and relate to both the highly vascularized nature of these tumors and their prominent surrounding edema (see Lamszus for further details). The implications of these findings are not yet clear but may relate to the increased incidence of the tumor in women, its tendency to enlarge during pregnancy, and an association with breast cancer. According to Rubinstein, they may arise from dural fibroblasts, but in our opinion, they are more clearly derived from arachnoidal (meningothelial) cells, in particular from those forming the arachnoid villi. Grossly, the tumor is firm, gray, and sharply circumscribed, taking the shape of the space in which it grows; thus, some tumors are flat and plaque-like, others round and lobulated. They may indent the brain and acquire a pia-arachnoid covering as part of their capsule, but they are clearly demarcated from the brain tissue (extra-axial) except in the unusual circumstance of a malignant invasive meningioma. Rarely, they arise from arachnoidal cells within the choroid plexus, forming an intraventricular meningioma. Microscopically, the cells are relatively uniform, with round or elongated nuclei, visible cytoplasmic membrane, and a characteristic tendency to encircle one another, forming whorls and psammoma bodies (laminated calcific concretions). A notable electron microscopic characteristic is the formation of very complex interdigitations between cells and the presence of desmosomes (Kepes). Cushing and Eisenhardt and, more recently, the World Health Organization (Lopes et al) have divided meningiomas into many subtypes depending on their mesenchymal variations, the character of the stroma, and their relative vascularity, but the value of such classifications is debatable. Currently neuropathologists recognize a meningothelial (syncytial) form as being the most common. It is readily distinguished from other similar but non-meningothelial tumors such as hemangiopericytomas, fibroblastomas, and chondrosarcomas. The usual sites of meningioma are the sylvian region, superior parasagittal surface of the frontal and parietal lobes, olfactory groove, lesser wing of the sphenoid bone, tuberculum sellae, superior surface of the cerebellum, cerebellopontine angle, and spinal canal. Some meningiomas- such as those of the olfactory groove, sphenoid wing, and tuberculum sellae- express themselves by highly distinctive syndromes that are diagnostic in themselves; these are described further on in this chapter. Inasmuch as they extend from the dural surface, they often invade and erode the cranial bones or excite an osteoblastic reaction, even giving rise to an exostosis on the external surface of the skull. The following remarks apply to meningiomas of the parasagittal, sylvian, and other surface areas of the cerebrum. The size that must be reached before symptoms appear varies with the size of the space in which the tumor grows and the surrounding anatomic arrangements. The parasagittal frontoparietal meningioma may cause a slowly progressive spastic weakness or numbness of one leg and later of both legs, and incontinence in the late stages. The sylvian tumors are manifest by a variety of motor, sensory, and aphasic disturbances in accord with their location, and by seizures. In the past, before brain imaging techniques became available, the meningioma often gave rise to neurologic signs for many years before the diagnosis was established, attesting to its slow rate of growth. Even now some tumors reach enormous size, to the point of causing papilledema, before the patient comes to medical attention. Increased intracranial pressure eventually occurs, but it is less frequent with meningiomas than with gliomas. However, it is also occurring with increased frequency in immunocompetent persons- a finding without evident explanation (although theories abound). For many years, the cell of origin of this tumor was thought to be the reticulum cell and the tumor was regarded as a reticulum cell sarcoma.
Syndromes
- Enlarged scrotum
- Spinal cord abscess
- Take the medicines your doctor told you to take with a small sip of water.
- Certain tumors
- A small tube (catheter) is often left in place. You can receive more medicine through the catheter to help control your pain during or after your procedure.
- Faintness
- The scrape is very large.
- Vitamin K deficiency
Pain and thermal sense are reduced more than tactile exotic herbals lexington ky order generic v-gel on-line, vibratory shivalik herbals purchase v-gel uk, and position sense (a "pseudosyringomyelic") pattern bajaj herbals fze discount 30gm v-gel visa. Autonomic involvement is another important characteristic- loss of pupillary light reflexes and miosis himalaya herbals uk 30gm v-gel amex, anhidrosis, vasomotor paralysis with orthostatic hypotension, alternating diarrhea and constipation, and impotence. Difficulty in walking also develops and has its basis in a combination of faulty position sense and mild muscle weakness. Cranial nerve involvement (facial weakness and numbness, loss of taste) is a late manifestation and occurs in only a few cases. A few patients have had severe amyloid heart disease from the onset (Ikeda et al). Weight loss may be pronounced, owing to anorexia and disordered bowel function and the later development of a malabsorption syndrome. Vitreous opacities (veils, specks, and strands) may progress to blindness, but this has been rare; in a few, there has been an impairment of hearing. In this and the following most common familial amyloidoses, the amyloid is derived from an inherited abnormality of serum protein transthyretin (formerly called "prealbumin"). In the originally described Andrade type, methionine replaces valine at amino acid 30; this has therefore been referred to as transthyretin amyloidosis. Familial amyloidosis with carpal tunnel syndrome (Swiss type) Falls and coworkers in 1955 and later Rukavina and associates described a large group of patients of Swiss stock living in Indiana who developed, in their fourth and fifth decades, a characteristic syndrome of acroparesthesias in the hands due to deposition of amyloid in the connective tissues and beneath the carpal ligaments. There was sensory loss and atrophic muscle weakness in the distribution of the median nerves, which were compressed. In some of the patients, other nerves of the arms were said to have become involved later. As with the Portuguese type, an abnormal transthyretin is the basis of the deposition of amyloid. Iowa type In 1969, van Allen described an Iowa kindred with onset, in their 30s, of a fairly severe sensorimotor neuropathy, involving the legs and then the arms. There was amyloid deposition in the testes, adrenal glands, and kidneys (the usual cause of death) as well as a high incidence of peptic ulcer disease. The amyloid in this disease is derived from apolipoprotein A-1, in which there is an amino acid substitution. Cranial neuropathy with corneal lattice dystrophy this unusual form of amyloid neuropathy was first described in three Finnish families by Meretoja- hence the label "Finnish type. Peripheral neuropathy may not be evident until the fifth decade, at which time the facial nerves, particularly their upper branches, become affected. The nerves of the limbs are involved even later and to a much lesser extent than in other amyloid neuropathies. In advanced cases there is a distinctive appearance of excessive skin folds about the face, facial diparesis, dysarthria, spasticity, and dense loss of posterior column function. At postmortem examination, deposits of amyloid are found in virtually every organ, but mainly in the kidneys and blood vessels and in the perineurium of affected nerves. The latter is normally an actin-binding protein, but it is also an important constituent of basement membranes, which may explain the deposition of amyloid in the cornea and skin. Diagnosis When the characteristic painful small-fiber type of sensory disturbance and autonomic changes are coupled with a family history of the same constellation, the diagnosis is not difficult. As noted in the earlier section on the acquired paraproteinemic neuropathy, the presence of a monoclonal (rarely polyclonal) immunoglobulin in the blood is found in only a limited number of patients with familial amyloid cases and it is of a low quantity, usually just above the upper limit of normal for the immunoglobulin subclass. Otherwise, as noted by several authors, the two types of amyloid disease are quite similar and, indeed, about 10 percent of cases thought to be acquired will in the end be found to have the genetic disorder (Lachmann et al). The situation has been rectified to some extent by the availability of gene sequencing to detect mutations related to amyloid. Such testing is justified if there is a low concentration paraprotein (or none) and a typical amyloidotic polyneuropathy and when the family history does not point to the correct diagnosis. Pathologic Findings Amyloid deposits are demonstrable in the walls of blood vessels, the interstitial (endoneurial) tissues of the peripheral somatic and autonomic nerves, and in the spinal and autonomic ganglia and roots. There is a loss of nerve fibers, the unmyelinated and small myelinated fibers being more depleted than the large myelinated ones. The anterior horn and sympathetic ganglion cells are swollen and chromatolysed due to involvement of their axons, and the posterior columns of the spinal cord degenerate, also on a secondary basis.
Cheap v-gel on line. Пустые баночки март 2019 CosRX Фаберлик Лореаль.